
Lean Six Sigma in Healthcare: A Case Study
Author: Eduardo Amezcua, Lean Consultant, Shingo Facilitator, and Black Belt
Most examples of Lean Six Sigma projects involve manufacturing processes. This is mainly because it was developed in that environment. But LSS is a methodology that works well in a variety of industries. It is increasingly being used in healthcare to improve quality of care and save on costs.
My interest in applying Lean Six Sigma goes back to an experience I had as a college student. While I was studying for my master’s degree I had to go to the hospital. I thought it was going to be a quick stop at the ER. As you might guess my visit took longer than expected.
The staff at the hospital worked fast to gather all my personal information. Then the waiting began. After nearly two hours I was still waiting to be seen by a doctor. Eventually I needed an IV and my stay at the hospital lasted for two days. It was at this point I realized I would write my master’s thesis on applying lean in healthcare.
The healthcare industry is fascinating. There are so many processes involved in taking care of a patient that I think sometimes not even hospital management realizes the true level of complexity they face. As a patient you do not want to deal with all the paperwork involved, all the time spent waiting on test results and doctors to make decisions. Plus the food isn’t very good. You wish you could just get well and leave.
As LSS practitioners we know it is important to go to the gemba, to observe the process, and to document the process through mapping. An analysis of a detailed map helps us to understand which steps are customer value add (CVA) activities. In healthcare – as in other industries – the percent of time doing CVA activities is minimal. The waste we find in healthcare processes will really open your eyes to do tons of improvement projects.
I‘d like to share an interesting case study in healthcare where the DMAIC methodology was used to solve a challenging problem. What I enjoyed the most about this example is how staff at the hospital worked along with engineers to improve the general process directly affecting patient care.
Background
In Italy there are around 100,000 hip prothesis surgical implant procedures performed every year. This represents a cost of €1.3 billion ($1.54B). This single procedure is a big expense in a country where healthcare is provided by the government. Healthcare costs represented 14.2% of the total public spending in Italy in 2012.
At the University Hospital ‘Federico II’ located in the city of Naples, Italy, they decided to improve their prothesis implant surgical process. They chose Lean Six Sigma as the approach to improve patient care and reduce costs. The ‘Federico II’ University is one of the oldest secular universities in Italy. The hospital has about 1,000 beds and is an important resource for southern Italy.
Define
First, the project team was formed with hospital staff from different areas including administrative, two surgeons, and three engineers. Yes, it was a very multiskilled team.
The team started by working on the project charter. They set a goal to reduce the hospital length of stay (LOS) to less than 14 days, on average, for this procedure. A counterbalancing goal was to maintain quality of care.
Next, they began working on the SIPOC. In creating the SIPOC the team decided to focus on the CARE PROCESS which consisted of administrative services. The team decided the actual surgery itself would be out of scope. In other words, the goal was not to change how surgery is performed but to eliminate all the waste around it.
Measure
The team decided to collect historic data from 19 months of admissions to the UOC Orthopedics and Traumatology Center. This represented a total of 79 patients who had this surgery performed during this period. The data was found to be normally distributed, with an average LOS of 18.9 days.
Analyze
The team decided to keep things simple. They developed a High-Level Process Map to identify value and waste. One that everybody could understand.
As part of the root cause effort the team invited other staff who played a role in the process for help. A group of nurses, physical therapists and anesthesiologists were asked to participate in a brainstorming session to determine possible reasons for the high LOS. By involving a mix of hospital staff with varying degrees of knowledge of the process they were able to get both an insider perspective and some good ‘external’ ideas.
Next, the team decided to create an Ishikawa (fishbone) diagram. Four main categories of root causes were identified:
- Patient
- Hospital staff
- System
- Process
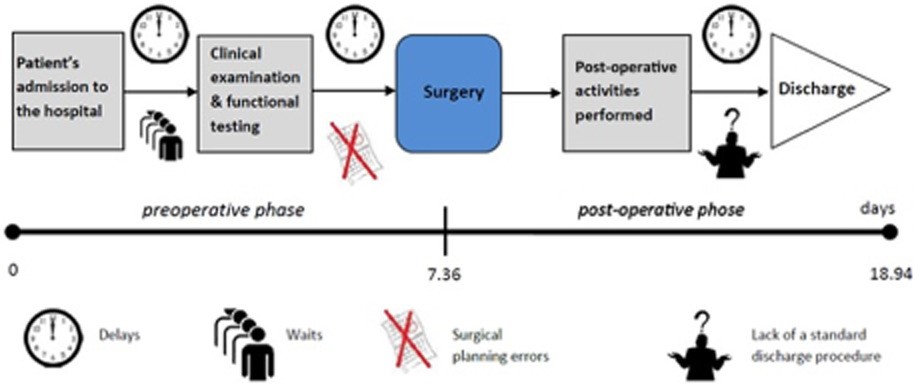
In Figure 1, we can see the very high-level process map the team created to show process flow:
Improve
The team brainstormed on potential improvements to the process. Some of the actions chosen may sound simple, but the key is they were changing the process to improve. As part of the Analyze Phase the team determined that patients were admitted to the hospital, and then had a surgery risk assessment performed. This assessment involved examinations plus diagnostic and laboratory tests. These activities could take days to complete.
To solve this “waste” the team implemented a pre-hospitalization service. With this new approach the patient goes through all the risk assessment steps without being hospitalized, prior to the surgery.
This is analogous to applying the lean concept of SMED (i.e., 4-Step Rapid Setup) involving moving internal setup activities to external setup activities. Using this approach, the surgery itself is the internal setup. By moving pre-surgical activities and post-surgical activities to external activities the length of stay could be shortened, and patients spend less time in the hospital.
The following table mentions some of additional root causes identified and the solutions implemented which were developed as part of the Improve Phase:
| Root Cause | Solution |
| Lack of standard discharge procedure | Standardization of the discharge process |
| Complex bureaucratic procedures resulting in compilation and communication errors among users involved in the process | The simplification of bureaucratic procedures |
| Wrong surgical planning | Optimization of procedures for the reservation of operating rooms |
| Preconceptions against the use of the health care information system | Promotion of the health care information system |
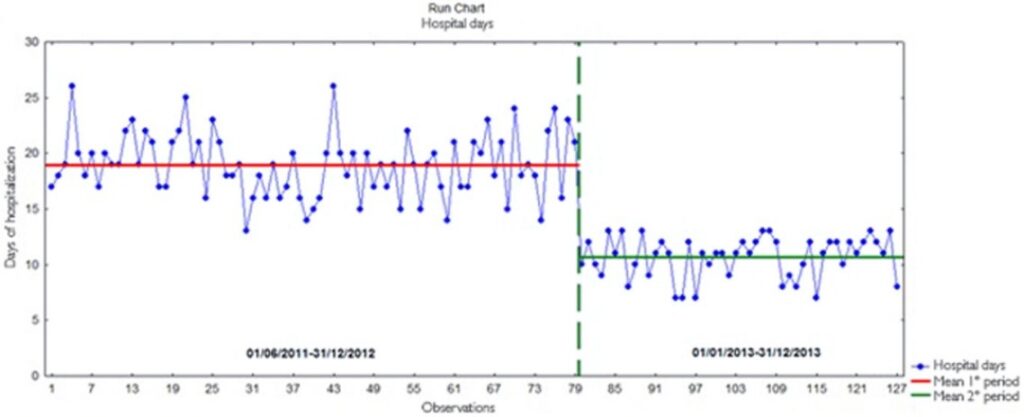
The team decided to run a pilot of the improved process which incorporated these improvements, along with other actions. If we observe Figure 2, it has two stages, the first stage represents 18 months of data. The second stage represents 12 months of data after the implementations were done. The length of stay was reduced from an average of 18.9 to 10.6 days – a 44% reduction! In addition, the variation in LOS was improved, with the standard deviation going from 2.9 to 1.8 days (38% improvement).
Control
To ensure the new, improved process was sustainable the team focused on three main areas:
- Periodical review of the implementation
- Internal audit checklist modified
- Run chart of LOS data which was updated periodically
As we can see, the hospital went beyond its original goal without compromising the heath of the patients. The average cost for a day in a hospital is €674. Assuming the same rate of implant surgeries, the estimated annual cost saving is around €260,000 ($307,000). The result obtained was great.
When you truly realize how much waste you have in your system you will surprised. But what is most gratifying – and leads to real culture change – is the satisfaction which comes from doing small improvements that have great results. Remember – Lean Six Sigma can be used in a wide variety of environments. It doesn’t matter if a product or a service process. There is always room for improvement.
Bibliography:
Cesarelli, Mario. “Lean Six Sigma: a New Approach to the Management of Patients Undergoing Prosthetic Hip Replacement Surgery.” Journal of evaluation in clinical practice. 21.4 (2015): 662–672. Web.
More about Eduardo Amezcua:
Eduardo Amezcua’s formal background training is in Industrial Engineering with a Master in Science (Quality and Productivity) with the proficiency to help companies improving and creating a continuous improvement culture. He has done industrial engineering projects in several industries such as food processing, ceramics, printing, beverage and software. He delivers training and consulting in manufacturing and service environments. Since a young age, he worked in multicultural environments in New Zealand, Mexico and USA.
